2.2. Calculation of temperature field2.2.1. Traditional method
By threshold segmentation of the speed of ultrasound image, tissue and its transitional area are separated by the following rule:


where v(x, y) is the speed of ultrasound at (x, y), v1 and v2 are average ultrasound transmission speeds in tissue1 and tissue2 respectively, Sm (m = 1, 2) are the areas of tissue1 and tissue2 and we suppose v1 < v2.
With the profiles between temperature and speed of ultrasound in tissue1 and tissue2, f1(v) and f2(v), temperatures in tissue1 and tissue2 can be acquired through

The SOS image mixes the speeds of sound of the two tissues at their boundaries due to the finite resolution of the imaging system, given by the system’ s line spread function (LSF), that is,

as the speed of sound in mixtures of homogeneous tissues follows a simple linear mixture model. Equation (7) gives a linear combination of the two different speeds at a sharp vertical boundary with a rectangular LSF. Thus, the measured speed v′ (x) in the transitional area would be
where Δ x = x2 − x1, Δ y = y2 − y1, and (xm, ym) (m = 1, 2) are the points in the boundary of the transitional area and tissuem.
The temperature at a sharp vertical boundary ideally would be given by a similar equation
We use the data of the speed of sound in the transitional area with a pixel and conduct the pixel calculation from the speed of sound. The temperature in the mixing area is expressed as

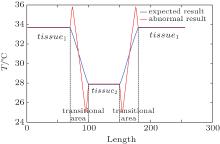
This provides distracting edge enhancement when the transitional area is not accurately segmented by Eq. (4). To illustrate this, suppose that a homogeneous tissue with low temperature is surrounded by a high temperature tissue. When tissues and their transitional areas are well distinguished and equations (6) and (9) are correctly applied, the temperature curve for the model is represented by the blue line in Fig. 1. However, if the boundary between two tissues is an unknown mixture of the two, equation (10) must be employed and even a sharp boundary will have the edge artifacts of the red line when the transitional area is segmented into tissues.
2.2.2. Proposed method with optimization
To allow for thin layers of mixed tissue and using Eq. (10), or one with a different LSF, continuity of temperature distribution is used as a constraint to rebuild the temperature image. After rough segmentation using Eq. (4), the boundary of the transitional area is determined by the following equation:

where dvm (m = 1, 2) is the average of the gradient of the speed of ultrasound in the identified tissue1 or tissue2:

The transitional area is denoted as D, and its boundary as L. Generally, we assume that the whole transitional area is segmented into two parts as Dm (m = 1, 2) by the boundary. Then thermal conductivity λ in each part is a constant. In addition, there is no inner heat source in each transitional area. Thus, equation (3) in each Dm is simplified into

Since the two transitional parts share the boundary, we can obtain the heat conduction equation of the whole transitional area, which is expressed as

Temperature at L as the boundary condition is calculated by Eqs. (11) and (12) and Eqs. (5) and (6) as follows:

The finite element method[41] is a numerical technique for finding approximate solutions to boundary value problems for partial differential equations. We divide the whole area of interest into similar parts called finite elements and use this method from the calculus of variations to solve the problem. In order to solve Eq. (14) with the boundary condition described in Eq. (15), the transitional area D is divided into m non-overlapped triangles e1, e2, … , em. For all m triangles, there are n non-overlapped vertices d1, d2, … , dm.
For triangle ei (i = 1, 2, … , m), coordinates of its three vertices are denoted as (xi1, yi1), (xi2, yi2), and (xi3, yi3). Equation (15) is used to calculate the coefficient matrix Kei:
where r, s, and t are the index numbers of the three vertices of triangle ei, and

The n × n matrix K is built by elements kpg from Kei:

Temperature of all vertices is acquired by solving:

where T = (T1, T2, … , Tn)′ is the vector of the temperature of all vertices. The temperature of vertices on boundary L is given by Eq. (15) as a known boundary condition.
2.2.3. Reconstruction quality evaluation
While rebuilding the temperature field image based on Eq. (14), we take the absolute difference between the temperature of one pixel and the mean temperature of its adjacent four pixels as a criterion to evaluate the smoothness of the rebuilding image, which is expressed as

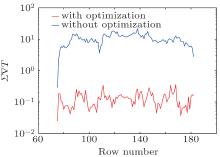
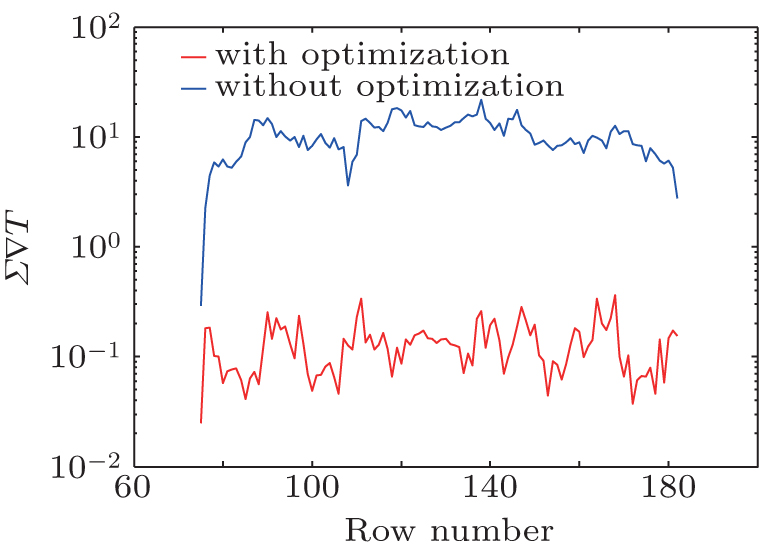
Bipolar edge enhancement artifacts are the abnormal results around the boundary. Mean variation of temperature of adjacent pixels in the transitional area, which is defined in Eq. (21), is calculated as a criterion to evaluate the image quality of the reconstructed temperature field, and is given as

where M is the total number of pixels in the transitional area.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 , Pinter Stephen Z.
, Pinter Stephen Z.